Defining the right problem
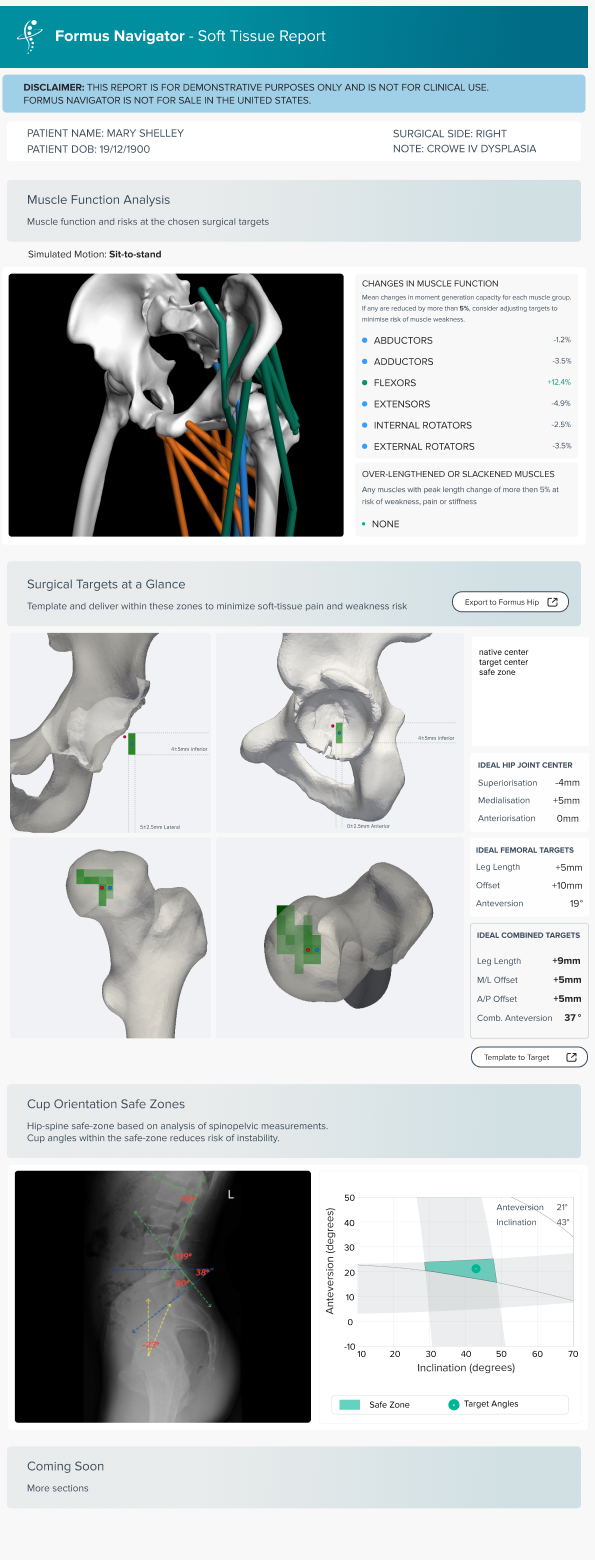
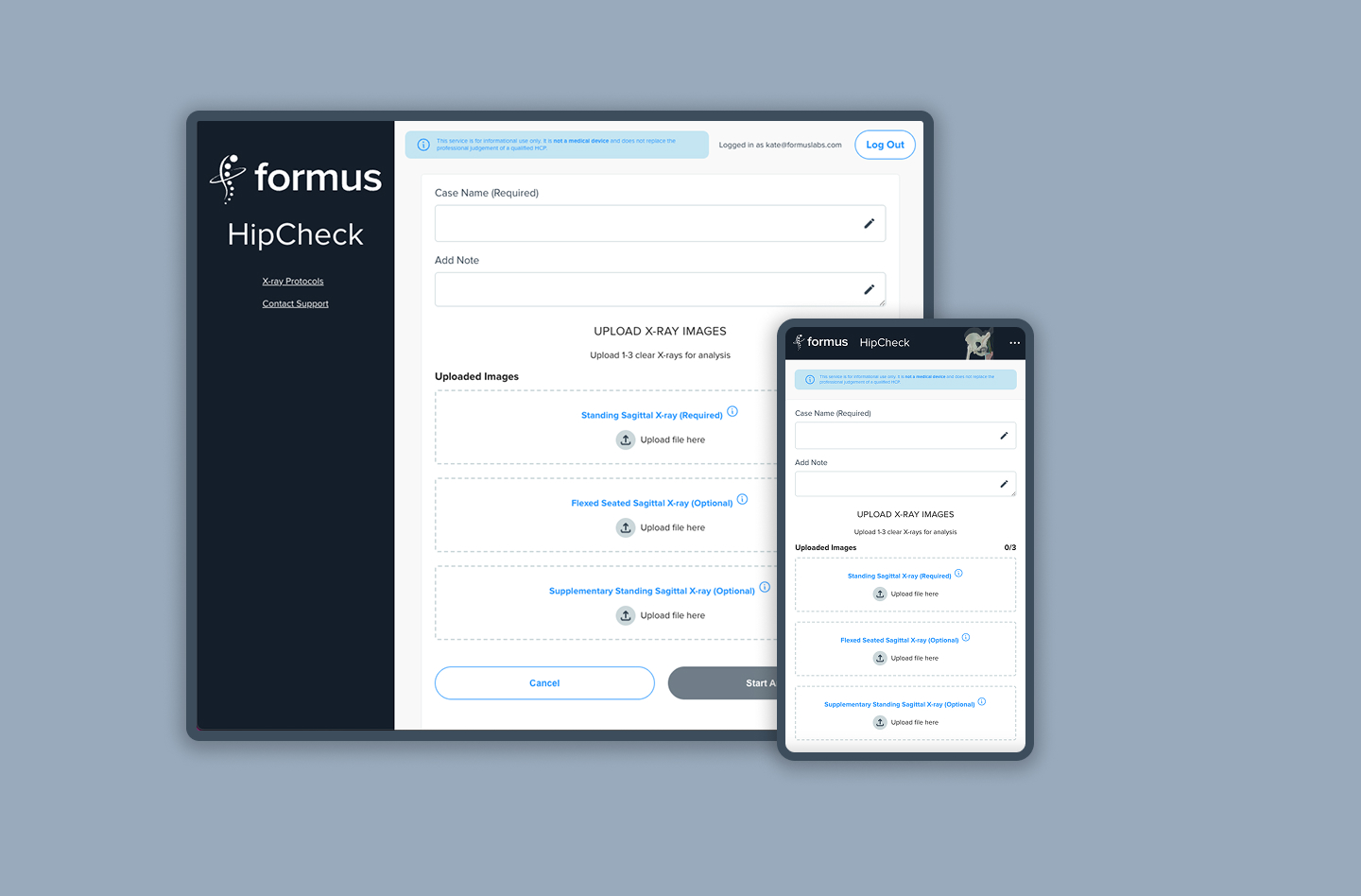
This shift reframed Navigator’s purpose. Instead of asking how much data we could show, the question became how little information we needed to confidently flag risk. The product moved toward answering a simple clinical question: is this patient at risk, and should I look closer?
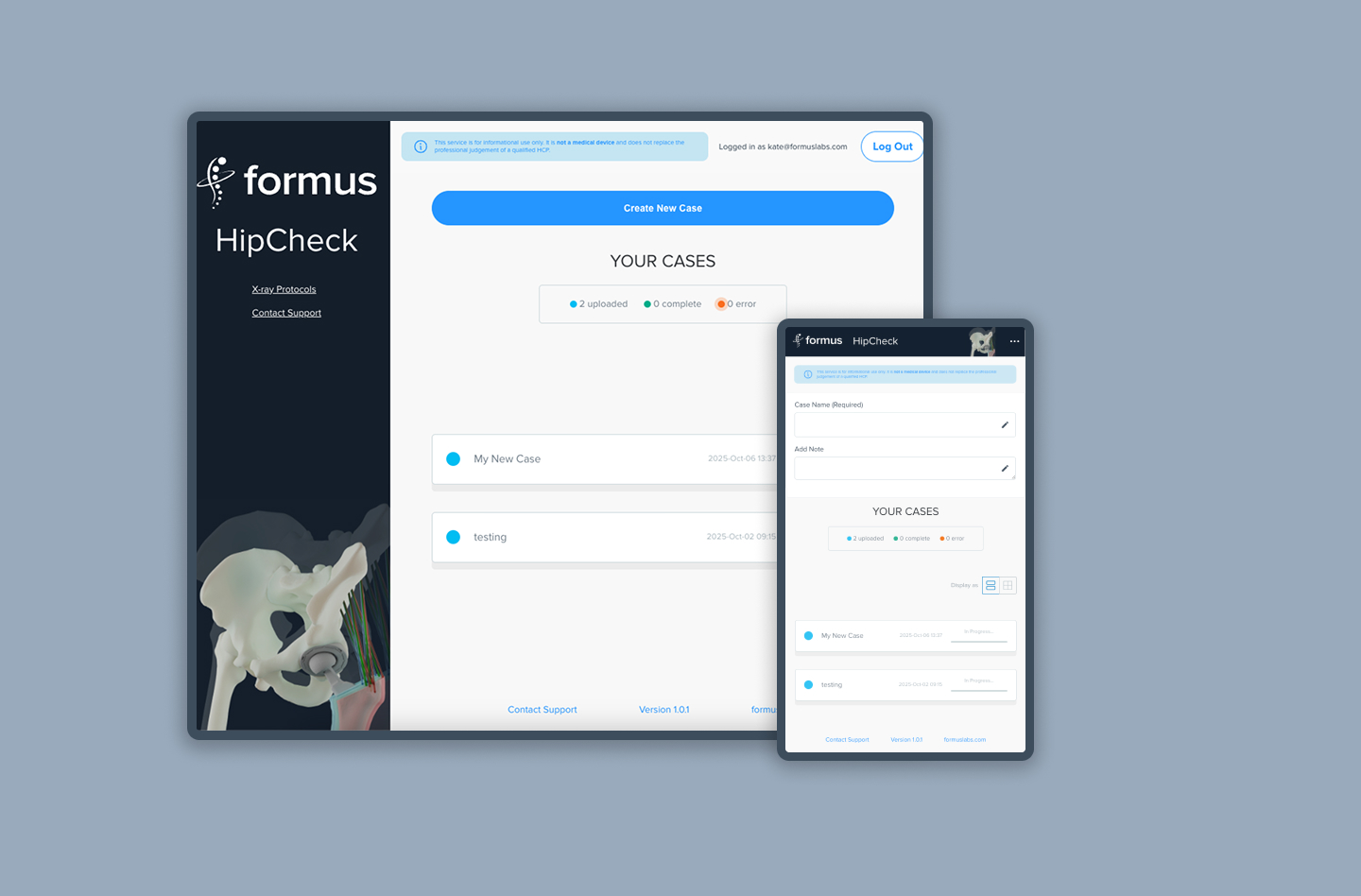
This reframing aligned the product with real surgical workflows and laid the foundation for trust. It also helped align stakeholders across research, engineering, and product around a shared goal.
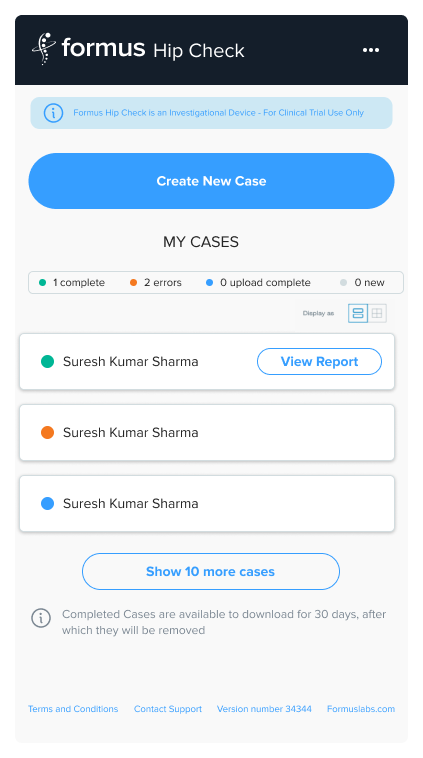
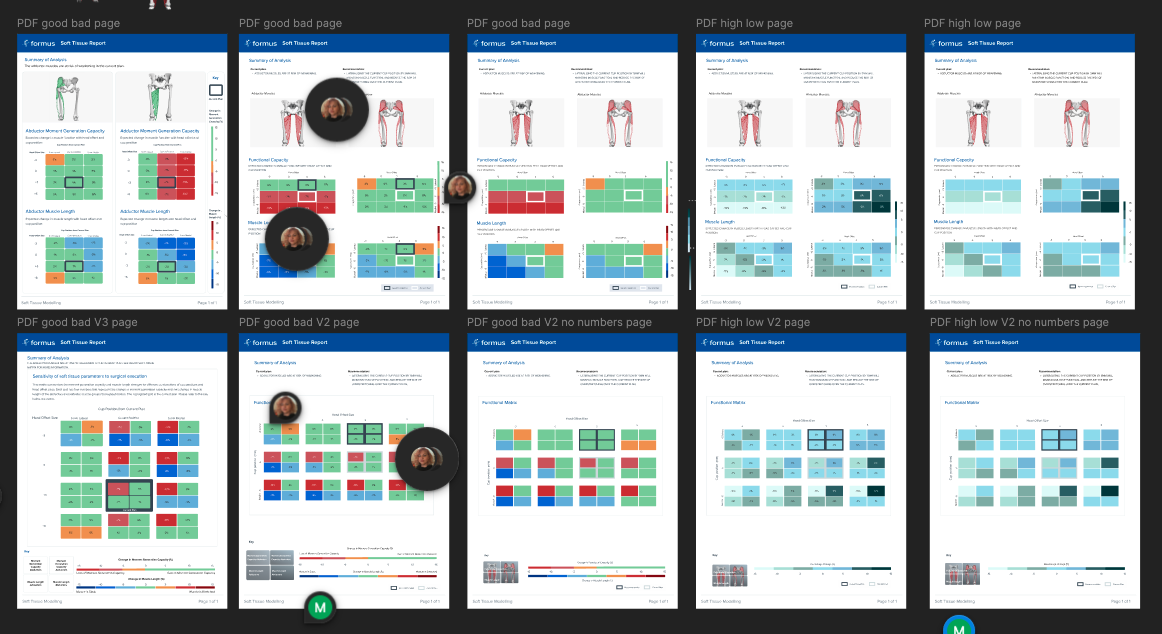
Iteration was continuous and research-led. Feedback loops with surgeons helped refine language, thresholds, and visual emphasis, ensuring the UI aligned with how risk is assessed clinically. The introduction of a traffic-light style system marked a turning point, allowing surgeons to scan results in seconds while still retaining access to deeper detail when needed.
Each design decision focused on balancing simplicity with credibility. The interface needed to feel clinically trustworthy, grounded in research, and defensible in a regulated environment.
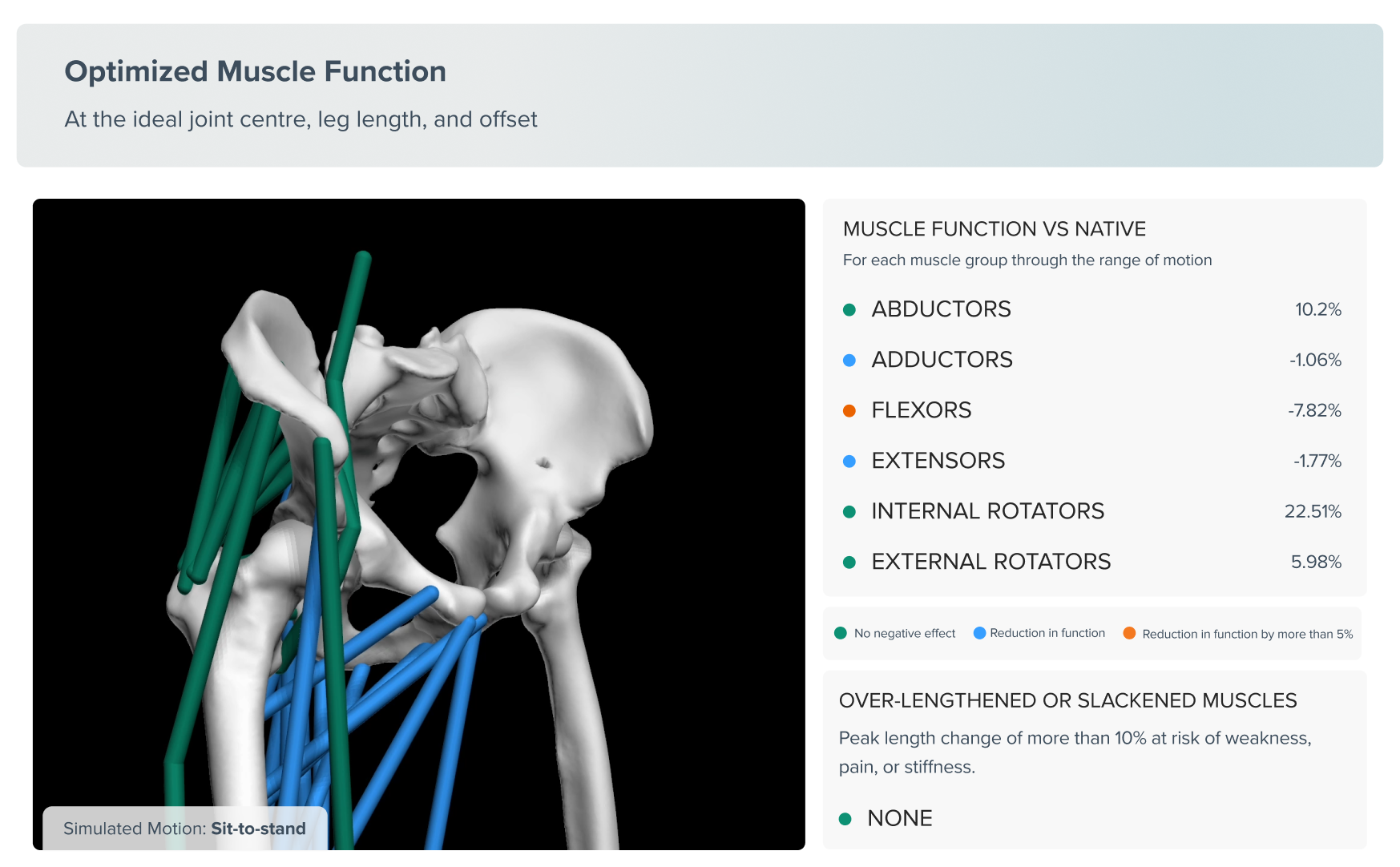
A core focus was enabling clinicians to understand the intent and reliability of automated recommendations.
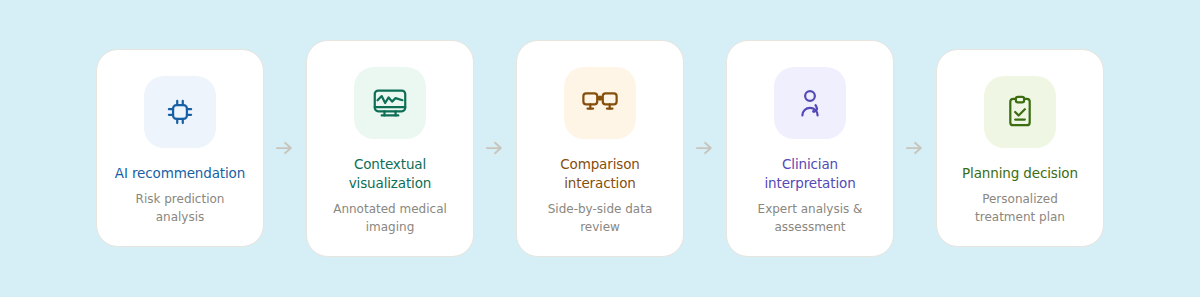
I explored interface patterns that communicated system certainty without overwhelming users with technical detail. This included progressive disclosure of supporting data, spatial visual cues reinforcing anatomical context, and interaction flows that allowed rapid comparison between manual and AI-assisted planning approaches.














.gif)
.png)
